Uterine Prolapse and Vaginal Prolapse for USMLE
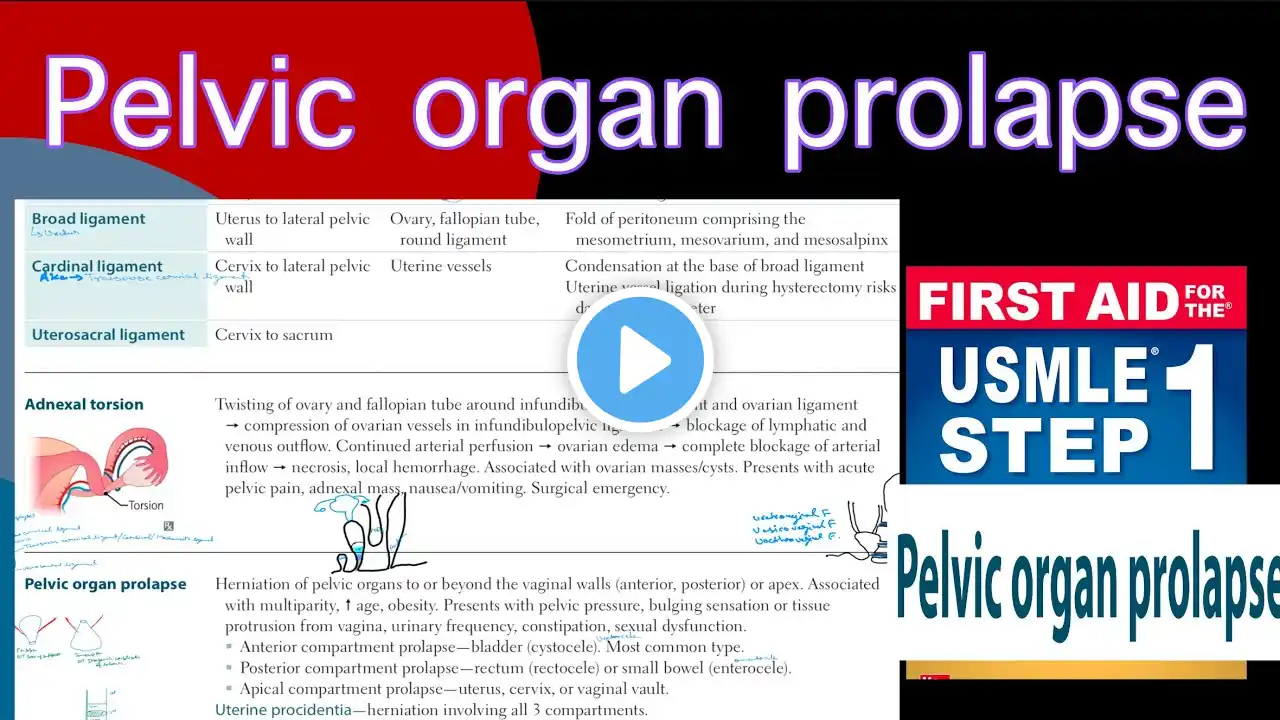
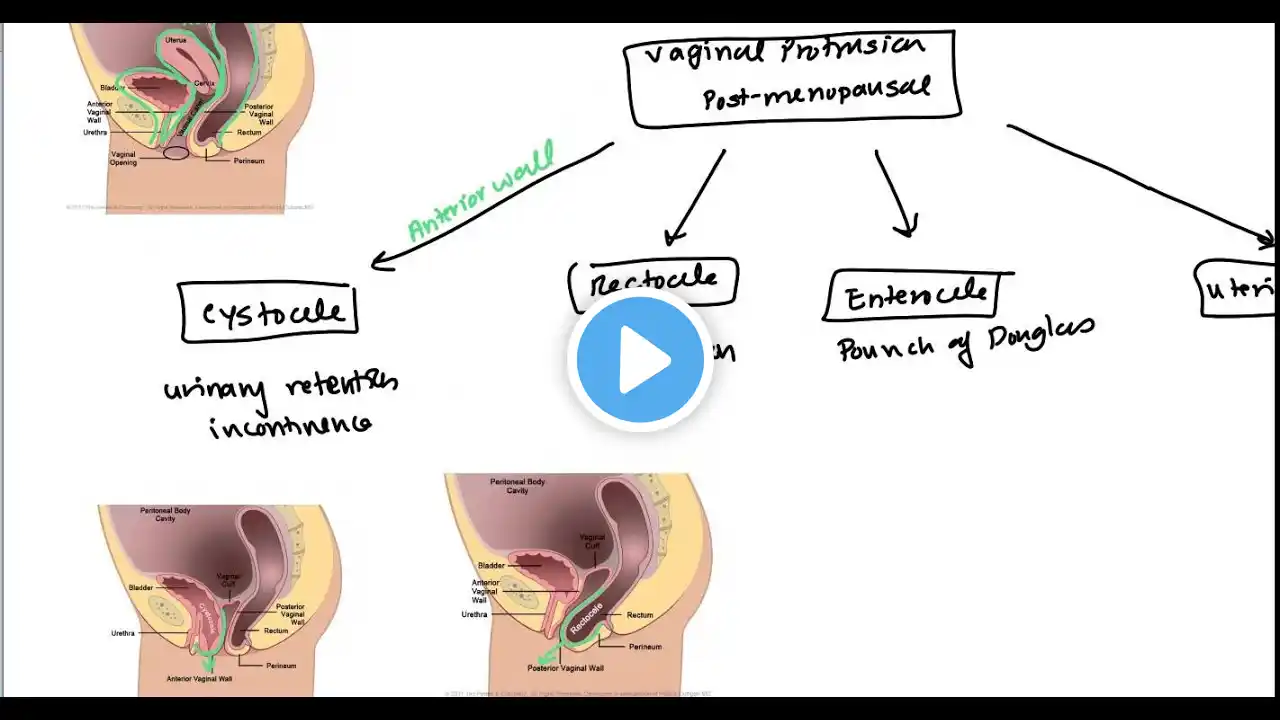
Uterine Prolapse or Vaginal Prolapse generally presents as a protrusion from the vagina in a post-menopausal woman. In the post menopausal period there is atrophy of vagina which increases the likelihood of protrusion. ANTERIOR VAGINAL PROLAPSE (CYSTOCELE) Bladder prolapses through the anterior portion of the vagina. Generally occur in patients with hysterectomy. Patient generally complains of urinary retention or incontinence. POSTERIOR VAGINAL PROLAPSE (RECTOCELE) Rectum prolapses through the posterior wall of the vagina. Patient usually presents with constipation or requires digital palpation in order to defecate ENTEROCELE The small intestine prolapses through the vagina through the pouch of Douglas. Patient symptoms will be bdominal pain associated with decreased bowel movements due to invovlement of Pouch of Douglas UTERINE PROLAPSE The uterus prolapses through the vaigna due to failure of the fascia that holds up the uterine organ. Severity is graded based upon how low the uterius protrudes. Grade 1 - Above the one half of the introitus. Grade 2- Below the half of the introitus. Grade 3- Protruding through the vagina Grade 4 - the entire uterurs prolapses through the vagina (Precedentia) Vague symptoms of vague pressure. Prolapse increases with standing and walking and decreases with laying down. Causes of Uterine or Vaginal Prolapse. Uterine prolapse can be caused by vaginal birth due to increase stretch especially if there is any type of forceps or vaccuum and it can tear and weaken uterine ligaments. Old age due to low estrogen that leads to atrophy and weakening the entire vaignal area. History of pelvic surgery leading to weakening. Increase pressure due to obesity and tumors. Treatment of Uterine Prolapse and Vaginal Prolapse Keigel exercise which contract pubococcygeus muscle. Estrogen if Post-Menopausal. Pessary whic his inserted into vagina and prevent prolapse of vaginal and uterine contents. Surgery such as hysterectomy and repair anterior or posterior wall of the vaigna.